The Eye and Vision
The human eye, a small orb with a diameter of around 1 inch, provides humans with much of the sensory information that we use on a daily basis. From walking to writing, dressing one’s self and even reading this paragraph, the eye is responsible for harnessing the visual world and translating it into a “language” that the brain can process to make decisions. Vision not only allows us to enjoy small pleasures like art and our favorite TV show, but it keeps us from harm— from allowing us to avoid walking off the edge of a sidewalk into a busy roadway to letting us evaluate whether the two week old bread in our cabinet is still suitable for consumption.
In order to understand how vision works, one must first understand the basic anatomy of the eye. After that, the logical connection is to understand how the brain interprets this information to form a picture. Once we have examined our light sensing structures, we will look at light itself and the regions of the spectrum that we can, and cannot, see. Finally we will address several visual problems and discuss how modern science and medicine are able to return or, in some cases enhance, vision.
Since a large portion of this unit does deal with anatomy, there are several regional and directional terms that are used to describe the position of different structures relative to one another. If you are unfamiliar with this terminology, it is highly recommended that you look at Appendix C, which contains a list of directional terms.
Anatomy of the Eye
The eye is made up of several important components that are directly related to the sensing of light. Many other components of the eye are responsible for supporting the organ with this primary function. Each part of the eye is described in detail below, and along with Figure 1, will provide adequate background information for teaching about this organ.
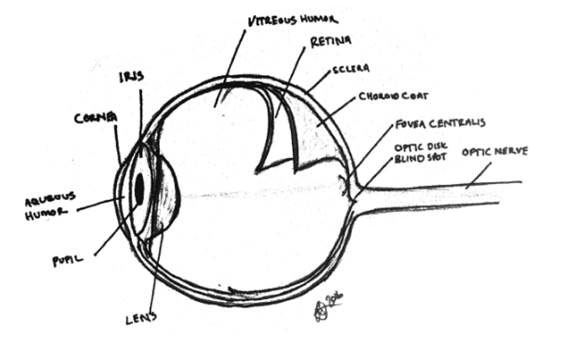
Figure 1. Anatomy of the Human Eye.
This illustration highlights several key structures of the eye. (Zullo)
The
sclera
, or the white of the eyes, is a tough, fibrous layer that serves many functions that are not directly connected to the sensing of light. This is the portion of the eye that provides shape and protects the other structures inside. The sclera is not the only structure that is responsible for protecting the eye, however.
In the medial anterior portion of the eye is a covering called the
cornea
. The cornea can be likened to a pair of goggles, since it provides further protection to the eye itself. It is relatively thick and strong—made up of five layers of cells—which are clear to allow light to pass through. This portion of the eye also serves a secondary protective function—it contains both pain and pressure (touch) sensory neurons that allow the eye to respond if it comes into contact with any foreign particles.
Behind the cornea, is the front, or the anterior chamber of the eye. The eye itself is not a single chamber. It is, in fact, two separate chambers divided by the lens. The anterior chamber is the front part of the eye. It is filled with a watery substance called
aqueous humor
. This slightly watery fluid helps provide the correct shape to the cornea and also to assist in light refraction. This fluid is constantly being replenished by special tissues called the ciliary processes—structures that are also responsible for suspending the lens. This fluid serves other functions as well, including providing amino acids and glucose to other parts of the eye for nutrition.
1
It is believe that the aqueous humor may also serve an immune function, as it contains immunoglobulins.
2
While the aqueous humor is responsible for bringing nutrition to a large portion of the eye structures, the eye itself is supplied with fresh oxygen and nutrients through the highly vascularized layer called the
choroid coat
. This tissue layer serves a second purpose of darkening the inner chamber of the eye to prevent light reflection. This layer is darkly colored because of the presence of melanin—which helps to absorb stray light from bouncing around the eye and prevents the development of macular degeneration by light toxicity.
3
In humans, the phenomenon known as photographic red-eye occurs when there is uncontrolled reflection in the back of the eye, highlighting the highly vascularized choroid coat and retina. Animals do not have this same “effect” and instead have eyes that may appear to glow due to a layer of melanin-poor tissue called the
tapetum
lucidum
. This structure, absent in humans, allows for animals to have strong night vision.
The colored part of the eye is made up of a muscle called the
iris
. Color of the eye is related to the amount of melanocytes that are found in the tissue. The more melanin, the darker the eye color appears. Melanin expression begins after birth when the
OCA2
gene is activated, which is why many babies when born have blue or lighter color eyes that may darken.
4
The iris functions much like the iris of a camera would. Its main function is to control the amount of light that is able to enter through the back of the eye through the
pupil
, or the hole in the center of the iris. Too much light to the back of the eye can cause damage and can obscure the surroundings.
Imagine walking out of a dark theater into a bright summer day. The bright lights can be painful and leave spots in front of your eyes. To compensate for too much light, your iris will constrict, narrowing the opening to prevent too much light from entering the rear or posterior chamber. In comparison, if you are sitting in a bright room and suddenly all of the lights go out, plunging you into darkness, your iris will contract, causing your pupil to dilate and allow additional light to enter. The same phenomena can be observed walking into a building on a bright day. Iris movements, and thus the size of the pupil, are controlled through antagonistic smooth muscles called the sphincter and dialator pupillae. A contraction of the spinchter pupillae closes the iris, making the pupil smaller while the dilator muscles open up the pupil.
The
lens
is located posterior to the pupil It is a disk shaped structure that is made up of concentric layers of cells that are laid down yearly The lens itself is elastic and can flex to allow the eye to focus on objects at different differences. The lens curved both assisting with this ability to focus. However, as the lens ages, these curves change and the iris becomes less flexible, casing age related vision problems such as far-sightedness. This is why, as adults move past middle age, they often require reading glasses when previously they did not.
As previously mentioned, the lens is supported by ligaments that are attached to the
ciliary
body
, a sublayer of the choroid body. These ligaments are responsible for helping to bend and flex the lens into the correct shape to allow for clear views at near and far distances. This process of bending the lens to shift between objects near and far is called accommodation, a phenomenon that will be discussed later.
Behind the lens is the posterior chamber of the eye. Like the anterior chamber, it is not hollow. The
vitreous
humor
, a jelly-like substance, fills this portion of the eye. It provides interior support to the sclera, aids in light refraction, and also keeps the layer called the retina in place against the posterior wall.
The
retina
is the sensory portion of the eye. Covering the back half of the eye, lying on top of the choroid coat. It is the most important structure for sensing light. As light passes through the lens, it is focused on the retina in the posterior chamber of the eye. This triggers specialized cells named rods and cones, which will be discussed in the next section concerning light sensing structures and the brain.
The retina is anchored to a single point to the back of the eye called the
optic disk
, were it leads into the
optic nerve
. This small spot in the eye lacks any rods and cones and thus, and results in the “blind spot”—a non-light sensing region of the retina. Finding the blind spot is a simple classroom activity that can be done with minimal supplies. Instructions for demonstrating the blind spot are located below in the section titled “suggested activities”. While the retina is anchored at one spot, it is possible for it to become detached at any point around the eye due to aging or physical trauma. During aging, vitreous fluid begins to shrink, allowing the retina to pull away from the choroid coat and tear, causing a loss of peripheral vision and further blinds spots
5
. Head trauma such as a blow to the head or whiplash from a car accident may similarly cause the vitreous humor to shift or leak. If this occurs, retinal tearing may also occur.
Light Sensing Structures and the Brain
As previously mentioned, the retina is the light sensing portion of the eye. Light flows into the eye past the cornea, through the pupil, and is focused by the lens on the retina which contains two light sensing structures called rods and cones. Rods and cones are both photoreceptors and are activated by different wavelengths of light. Rods are responsible primarily for scotopic vision, meaning they are active in low or dim light. For example, when walking around at dusk or stumbling around a darkened room one relies more heavily on the rods of the eye than the cones. These light sensing structures are more numerous than the cones and are found in greater angular separation from the fovea centralis. These structures have low spatial acuity, meaning that they are not able to strongly detect shapes of objects. Rods are missing entirely from the fovea centralis.
It is believed that the function of rods is a survival feature—they provide vision in low light environments including night vision, are sensitive to motion detection, and provide us with our peripheral vision
6
. These traits are important in allowing the eye to quickly sense danger approaching from the side, allowing for us to react. For this reason, the rod does not need to have high visual acuity—we do not need to know what
exactly
is coming but merely that something
is
coming
—
to serve its purpose.
Cones are activated during times of phototopic vision or high intensity light, and are also responsible for the detection of color along the visible light spectrum. Cones are highly concentrated (up to 1.5x10
5
cones/mm
2
)
7
in a region of the eye called the
fovea centralis,
a subcomponent of the macula lutea in the retina. This area is found just lateral to the optic disk and is the area where light is directed. There are three types of cones in the human eye, able to sense short, middle and long wavelengths of light (S-cones, M-cones, and L-cones, respectively). Each type of cone is photosensitive to different areas of the spectrum due the differences in the photopigments that they have. For example, S-cones are more highly active in the blue ranges of light, M-cones in the green ranges, and L-cones in the red ranges.
8
This does not mean that these cones are sensitive to only that particular range. The spectrum of these cones are overlapping, allowing them to perceive a wide spectrum of colors in response to the particular ratio of each that are active.
Unlike rods, cones are in areas for high visual acuity. The fovea centralis and the macula lutea are both highly focused areas, allowing for sharp details. This portion of vision allows for humans to focus on specific objects.
When light is focused on the retina, a photoreceptor chemical called rhodopsin is activated. This activation excites sensory neurons that are attached to the rods and cones, generating an electrical impulse. This impulse is channeled into the optic nerve which leads out of the optic disk and into the optic chiasma, a portion of the brain where the two optic nerves physically cross, located on the ventral or bottom side of the brain. Once in the optic track these signals are sent to the occipital lobe of the brain to be interpreted.
Vision and the Light Spectrum
Visible light comprises one part of the electromagnet spectrum. Electromagnetic wave frequencies depend on the number of cycles that travel through a specific point per unit time. The number of these cycles that pass through the point per second is measured in hertz (Hz). The visible light spectrum ranges from 75x10
14
Hz (400 nm) to 4.3x10
14
Hz (700 nm).
9
More commonly, visible light is described in terms of wavelength, which varies inversely with frequency. For example, 75x10
14
Hz corresponds to a wavelength of 400 nm, and 4.3x10
14
Hz is 700 nm.
There are several important functions of light that contribute to vision. Reflection, refraction, and dispersion will be discussed in this section.
Reflection assumes that light will travel as a straight line or ray until it hits a surface. Once it hits that surface it is absorbed and emitted from that material. This type of behavior is described with the ray theory of light, and ignores many of the wave principles that will be discussed later. On a smooth surface without any inclusions, such as a mirror, light will be emitted in a ray with the same angle as it hit the surface, and is known as specular reflection. Inclusions which result in a rough or irregular surface will cause diffuse reflection where the angle at which the light is emitted is different from the angle it hit the surface.
10
Reflection allows our eyes to see. When light hits an object, specific wavelengths of light are absorbed. Some of these wavelengths are emitted back by the object depending on the photopigments that are in it.
11
For example, the grass appears green because the wavelength that corresponds to green light is
not
absorbed. This light is released and it is absorbed by the cones in the eye, triggering “color” vision.
Refraction occurs when light impinges upon a transparent surface. When this occurs, light is “bent.” That is, when light travels from one medium (air) into a second medium (liquid) that have different refractive indices, a straight object such as a pencil that is placed in the liquid appears bent or disjointed.
12
Because of the differences in speed through the two media, the light appears to bend, and this can be used to determine the refractive index of a material or substance. For example, the refractive index through air is 1.000 and the refractive index through the aqueous humor is 1.336.
13
Several eye conditions exist because of refractive errors. If the eye itself is too long or too short, light is unable to focus on the retina. If the eye is elongated, light will be focused before the retina, causing nearsightedness. If the eye is shortened, the image will focus behind the eye causing far sightedness after accommodation. Both of these cases can be treated by using lenses to refocus the light on the correct place of the retina.
Astigmatism occurs if the cornea itself is distorted. Astigmatisms or uneven lens surfaces may cause the light to scatter slightly, leading to blurry vision.
14
In astigmatism, the eye is unable to evenly focus light because the cornea has an uneven surface. As the cornea is irregularly shaped, the light passes through the cornea at different angles, causing the image focused on the retina to look blurry or distorted.
15
Medical Interventions: Near and Far Sightedness
As with any organ there are instances where the body is not able to operate optimally. This section discusses some of the interventions that are currently used for various eye impairments that have occurred as a result of physiological defects.
The first set of interventions will apply to near and far sightedness and how we can use concave and convex lenses to redirect the light to the correct location of the eye. In cases of myopia, the subject is able to see objects that are near, but objects at a distance are blurry. This occurs because the image is focused in front of the retina before the fovea centralis. In order to correct this, glasses with diverging lenses are used which move the light back against the retina. The opposite is true in hyperopia or people who are far-sighted. They are able to see clearly at a distance but have difficulty looking at objects close up. This is because the image would be focused “behind” the eye, past the retina. Converging lenses cause the light to focus sooner than it would normally, allowing for clearer vision
16
.
Two of the most innovative medical interventions include colorblindness correcting glasses and the bionic eye.
Colorblindness is a condition where the eye’s color sensing cones do not correctly detect their normal corresponding wavelengths of light. There are several forms of colorblindness and it is often passed down through sex-linked inheritance. As such, colorblindness is more often found in men than women. One of the most common types of colorblindness is deuteranopia, more commonly known as red-green colorblindness.
In deuteranopia, the eye has difficulty sensing light in the green wavelengths because the M-opsins are misshapen due to a genetic abnormality on the X chromosome. Instead of picking up “green” they respond more strongly to the longer wavelengths that correspond with orange or red. This often causes a muddying of colors and the inability to distinguish red and green wavelengths. This will not only affect the ability to perceive these two colors, but most colors in the perceivable light spectrum. Since both red and green cone are triggered, the colors might appear to be a muddy yellow color. For examples of what different types of colorblindness might look like to someone who is experiencing them, visit the resources section below.
Recently, a new type of corrective glasses on the market, released by the company EnChroma, helps to restore some of the color spectrum to people who are red-green colorblind. These glasses work by filtering out light that falls between 550 nm and 570 nm—a range of the spectrum that is usually just outside of the range of a normal green cone.
17
By filtering out these wavelengths of light, the green cone is, essentially, shifted back into a normal range so it is not excited inappropriately. This filtration of stray light fixes the signal coming into the eye, allowing green cones and red cones to be excited at the correct times and the eye to interpret these stimuli as the correct colors. A link to their website is listed below in resources.
The last intervention that will be discussed in this section is the bionic eye. While this may seem like something out of a science fiction movie, bionic eyes have become a reality for people suffering severe retinal damage. In patients who have lost the ability to sense light, retinal implants are used as a substitute.
Patients are fitted with a pair of special glasses that have a video camera embedded in the side. The camera captures the image and sends wireless impulses to the back of the retina where a sensor has been implanted.
18
These signals stimulate the optic nerve similarly to how the rods and cones would be directly stimulated by light. The eye is then able to send this signal to the brain for decoding.
The Ear and Sound
Our eyes are not our only way to sense the world around us. Hearing and the ability of people to perceive sound is also a critical way for humans to understand and evaluate the world around them. Sound provides us with valuable information and a richness to our sensory interpretation of our environments. For most humans and animals, sound is a critical source of communication. Not only does hearing allow us to interpret a string of vocalizations together to create words, but it also allows us to hear the tone and timber behind the things people are saying—providing us with information about the inflection behind those words. Our ability to perceive sound provides us with information that we may not even notice initially. For example, the human ear is able to discern the difference between hot and cold water when being poured.
19
Anatomy of the Ear
The ear comprises three main areas: the outer, middle, and inner ear, all of which assist in hearing to some degree. In this section, the structures of the ear are described in the same order that sound travels through them (Figure 3).
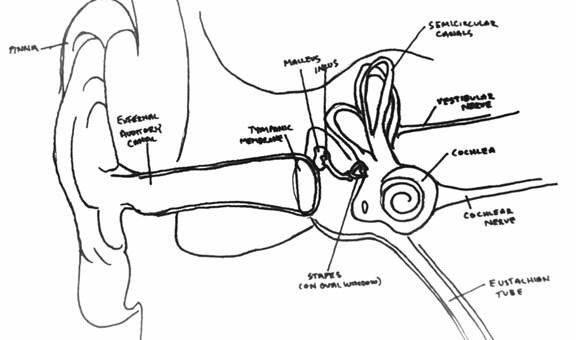
Figure 3. Anatomy of the Human Ear.
This illustration highlights several key structures of the ear. (Zullo)
The outer ear is what many people think of when we talk about ears, but the ear actually extends into the skull far deeper than we might imagine. The fleshy part of the outer ear is the
pinna
and it is responsible for directing sound waves towards the auditory canal. Think of the pinna as a funnel for sound, helping to focus sound waves inward.
Just past the pinna is the
auditory canal
. Like all orifices open to the outside world, this structure has a few forms of protection to prevent the collection of foreign particles and to help keep pathogens at bay. The auditory canal uses sebaceous glands to secrete a substance called ear wax, or cerumen. Ear wax not only assists in keeping foreign particles away from the middle and inner ear, but it also helps to keep the ear dry by providing a water barrier.
20
Just past the auditory canal is a membrane called the
tympanic membrane
or the eardrum. This structure serves as the divider between the outer ear and the inner ear. In the presence of sound, the tympanic membrane will vibrate. These vibrations are what is collected and transmitted through the rest of the ear and into the brain for decoding.
The middle ear, just posterior to the tympanic membrane, holds several important structures. This small portion of the ear is located adjacent to the temporal bone of the skull and connects with the
pharynx
or throat. This is often why some people may experience tickling sensations in their throat when they have tickling in their inner ear. This chamber of the ear is pressurized, with the
eustacian tube
serving as a way of helping to maintain the same atmospheric pressure as the environment.
There are three small bones, or
ossicles
, in the middle ear which are responsible for collecting and transmitting the sounds from the tympanic membrane. The
malleus
,
incus
, and
stapes
(or hammer, anvil, and stirrup). The malleus is positioned so that the proximal end is at the tympanic membrane and the distal end is free to swing much like a hinge. When vibrations hit the tympanic membrane, the malleus strikes the incus which is fused to the stapes. The vibrations travel through these two bones and enter into the inner ear, where the stapes abuts the cochlea.
21
The ossicles of the middle ear serve a very important function by helping to channel the vibrations in sound past the air-fluid interface of the outer and inner ear. The hammering of the malleus causes vibrations that are able to travel through the cochlea. It is estimated that, without these ossicles serving as an intermediary, about 99.9% of the energy from sound waves would be prevented from reaching the inner ear.
22
The inner ear itself is deep within the temporal bone of the skull. As previously indicated, the main structure of the inner ear is a fluid filled chamber called the
cochlea
. This organ is shaped like a snail. The large, “shell-like” portion of the cochlea is actually a tube filled with fluids called the
cochlear duct
. When the malleus strikes the incus and sends vibrations through the stapes, these vibrations impinge on the
oval window
, a thin membrane. The force is transferred from the bone, through the oval window into the fluid filled environment of the cochlear duct. Delicate cells called the
organ
of
Corti
are stimulated by these vibrations. Much like the rods and cones of the eyes, these cells are attached to sensory neurons. The sensory neurons transmit their signal along the
cochlear
nerve
into the temporal lobe of the brain, where sound is interpreted.
The inner ear serves a secondary function in addition to being able to transmit sound. Opposite the cochlear duct is a series of loops called the semicircular canal. These structures also contain a gel-like liquid called endolymph and hair like cells. However, instead of being activated by sound, as the head tilts side to side, the endolymph acts as a liquid level.
23
These impulses are sent to the cerebellum in order to help with balance and body positioning.
Sound and Sound Waves
Sound is generated in waves when a disturbance disrupts the medium. For example, consider a tuning fork. Tuning forks are composed of two short tines and a long stem. When this tuning fork is struck, the two tines push together and pull apart causing compressions and rarefactions in the air. These compressions act as “ripples” that are passed on through the air from the source of the disturbance. The sound that we hear is a based on its vibration frequency.
24
Frequency is classified as the number of oscillations within a given second—the number of times that this wave is being generated. The unit of hertz (Hz) is the number of those waves that occur per second.
25
For example, a tuning fork at 512 Hz goes through that many cycles per second.
Sound is a longitudinal wave, which means that both the particle motion that is generated and the velocity are traveling in parallels from the source. Sound is able to travel through gas (air conduction), liquids, and even thin solids depending on how elastic the medium.
26
Sound cannot travel through vacuum. A medium is required which could be a gas, solid, or liquid.
There exists a sound spectrum, similar to the light spectrum previously discussed. Sounds below 20Hz are considered infrasonic. Sounds in the infrasonic region might include the noises that occur during earthquakes, tsunamis, and other weather disturbances. There is some indication that, while humans are unable to hear at these frequencies, animals like elephants and cattle are able to detect these sounds and respond to them.
Sounds above 20 kHz are considered to be ultrasonic. Ultrasound is considered to be above the range of hearing for humans, but it is an important diagnostic tool in medicine.
27
Ultrasound frequencies can be used as an alternative to X-rays. It operates in a similar process to echolocation—sound is bounced off of the object and collected by computer devices to form pictures. Dog whistles used for training operate at ultrasonic frequencies.
When discussing sound, there are several important relative terms. Often, we use the term volume for sound. Loudness, however, is relative. For example, if you spend time with someone who has moderate to severe hearing loss, the volume on their TV, radio, or other auditory devices may be turned up to levels that are painful for a person who has normal hearing. For this reason, the physical quantification of sound is done is known as intensity. Intensity is measured in joules per second (J/s) through a square meter.
28
As the sound propagates further from the source, the intensity decrease since it is spread over a larger area. Decibels are a much more commonly used term for classifying intensity of sound.
The human range for hearing is between 20 Hz and 20 kHz. In the human auditory range, sound intensity is discussed in decibels, or db. To provide some prospective, a whisper is around 30 db, average conversational speech is at 60 db, and a concert with amplifiers is near 110 db. Exposure to noises more intense than 90 db for prolonged periods of time can cause hearing loss. Decibels are on a logarithmic scale. Every 10 db is a factor of 10 larger intensity, so something that is 60 db is 1000 times louder than 30 db (and a concert at 110 db is 100,000,000 times louder than a 30 db whisper).
29
Hearing Tests
There are several tests that can be used to identify hearing loss, both conductive and sensorineural. Conductive hearing loss is defined as difficulty in conducting sound from the outer through the middle ear. Often times, there may be a problem with either the tympanic membrane or the ossicles as these structures are responsible for conducting sound from the environment. Sensorineural hearing loss is characterized by problems in the cochlea, where sound is unable to be captured or conducted along the nerves. These tests are often performed by an audiologist, or a medical professional who is trained in ear, nose, and throat (ENT) diseases. The tests described below are all tests that can be performed by students in a classroom, but it is important to recognize that, unless performed by a professional in a controlled sound environment, these tests are not considered diagnostic.
The Rinne test is performed in order to look for differences for problems in conductive hearing. This test is use to look for differences in a single ear (unilateral) and requires the use of a tuning fork. This test works by comparing the ability to perceive sound that is transmitted by air conduction as opposed to sensorineural hearing. For this reason it is important that this test is completed in conjunction with additional testing.
To complete the Rinne test, a 512 Hz tuning fork is struck and held against the mastoid bone proximal to the ear of interest. The patient is instructed to indicate when they are no longer able to hear the sound to signal. At that point the tuning fork is moved next to the auditory canal. Again, the patient is instructed to indicate when they can no longer hear it.
In normal hearing, air conduction lasts longer than bone conduction, meaning that a person should hear the tuning fork for roughly as long or equal to the length of time they were able to hear it at the mastoid. If this is not the case, the following scenarios could be possibilities: If the conduction is longer at the bone than it is by the auditory canal, this could be indicative of conductive hearing loss of the outer and middle ear. A second possibility is indicative of sensorineural hearing loss, where both bone conduction and air conduction are decreased. In this case, the bone conduction may still be longer than the air conduction, but both durations are less than would be expected in normal hearing.
A second test that is often used to identify hearing loss is a pure tone test. This test generates a graph called an audiogram. In a pure tone test, an audiometer is used to play beeps at different frequencies and decibels. A graph is generated based on the threshold needed to hear the sound. This test can also be used to test for differences in air conduction vs bone conduction.
The audiogram is usually run at frequencies between 250 and 8000 Hz and two lines are generated, graphing the thresholds. Normal hearing can usually sense tones in the range of 0-20 db while moderate hearing loss thresholds are increased to 41-55 db. Anything between 71-90 db is considered to be severe hearing loss.
30
Aging and Hearing
As adults age, presbycusis or age related hearing loss, may occur. According to the National Institutes of Health, one of every three people between ages 65 to 74 experiences some form of hearing loss. This number increases by age 75 to nearly 1 in 2 adults. This hearing loss is usually bilateral and is gradual.
31
As a result, many adults may have difficulties hearing tones in the higher or lower frequencies. This might manifest as the inability to clearly hear the voices of children or women who tend to speak in higher octaves, or not being able to hear the phone ring. Many adults lose the ability to hear frequencies above 16 kHz, including the sound of a mosquito.
32
Presbycusis can be caused by several environmental factors. Adults who work in an occupation that requires them to be exposed to long periods of noises may experience hearing loss at specific frequencies. In addition to prolonged periods of noise, noises at high decibel levels can also cause hearing loss. In these cases, a single exposure may be enough to cause damage.
33
Medical Interventions: Hearing Aids and Cochlear Implants
There are two medical interventions that often arise in conversations about hearing loss—the hearing aid and the cochlear implant. Both of these devices allow someone who is hard of hearing or deaf to have some sound returned, however the way they operate are very different.
Hearing aids are small external devices that fit just inside of the auditory canal, much like an ear bud on a set of head phones would, or sometimes behind the ear. Hearing aids amplify sound, by increasing the vibrations that are entering the patient’s ear. The first part of the hearing aid is a microphone, which picks up sounds. These sounds are then converted into an electrical signal that passes through the amplifier. The amplifier boost the “volume” of the sound by increasing the impulse’s power.
34
This signal is then released into the auditory canal through a speaker
35
where the ear interprets the newly augmented soundwaves.
Since the hearing aid relies on the ear’s ability to pick up the signal that is sent into the cochlea, it is important that at least some of the delicate hair cells that make up the organ of Corti are still functioning. If there is too much sensorineural damage, then other medical interventions must take place.
Hearing aids take advantage of the ears natural processes by just providing a stronger set of vibrational waves for the inner ear to interpret. Cochlear implants, however, do not rely on amplification of sound at all. These implants are used to bypass the middle and inner ear exchange all together in order to deliver sound waves directly to the auditory nerve.
36
Cochlear implants are more invasive than a hearing aids since they require an implant to be incorporated directly into the head. This device, however allows patients who are deaf, or nearly so, to hear when a hearing aid would not be sufficient. In these cases, the inner ear is usually malformed or too severely damaged to transmit a signal along the auditory nerve.
This device works using a similar system to the hearing aid. A microphone that is in the external portion of the cochlear implant is responsible for picking up surrounding noises. Those noises are then sent to a speech processor which is found outside of the ear. This small computer converts the found to signals that the transmitter on the outside of the skill passes to the magnetic receiver implant that is found inside of the head, just superior to the ear.
37
This receiver takes the signal and coverts it into an electrical impulse that travel through electrodes into the electrode array that is directly linked to the auditory nerve.
This system allows the sound to bypass the ear altogether and can be one of the only treatment options for children and adults who are profoundly deaf. However, because there is no way to completely replace the number of nerve hairs that are found in the cochlea, this implant is not a perfect solution. The small array of electrodes is trying to do the job of thousands of hair cells. For this reason, patients often rely on sign language and lip reading to supplement the information that they are able to obtain from the cochlear implant.
Furthermore, there is a large amount of cultural bias for and against the implantation of hearing aids. Members of the deaf community are strongly against infant or toddler implantation because it removes that child from deaf culture. Many feel that being deaf is not something that needs to be fixed, but rather an aspect of one’s self that should be embraced.
Often, children who receive cochlear implants adapt well enough that they are able to interact with the world much as a hearing child would be able to. They grow up learning how to use the information from the cochlear implant and lip reading to give them a good picture of the auditory world around them. Parents in the hearing community who have a profoundly deaf child may never allow their child to develop the skills of ASL that would allow them to communicate with members of the deaf community.
38
Deaf parents who choose to have their deaf child implanted often face criticism from the deaf community since it can be seen as robbing their child of their culture. Since a strong emphasis is put on oral communication rather than just ASL, children could grow up experiencing a different language from their parents and relatives. The movie
Sound and Fury (2000)
explores this difficult decision as deaf parents of a deaf child must decide whether or not to have their children receive the cochlear implant. More about this movie is found under the sample learning activities and the resources tab.